REVIEW
A cura della Redazione della rivista “Medicina Multidisciplinare”
Electrochemotherapy in treatment of tumours
G. Sersa a, D. Miklavcic b, M. Cemazar a, Z. Rudolf a, G. Pucihar b, M. Snoj a,*
a Institute of Oncology Ljubljana, Zaloska 2, SI-1000 Ljubljana, Slovenia
b University of Ljubljana, Faculty of Electrical Engineering, Trzaska 25, SI-1000 Ljubljana, Slovenia
European Journal of Surgical Oncology (EJSO) 2008; 34: 232-240.
Introduction
Electrochemotherapy is a local treatment which combines treatment with chemotherapeutic drugs and tissue electroporation, i.e. application of short, intense electric pulses to the tumour. Application of electric pulses potentiates the cytotoxicity of chemotherapeutic drugs by permeabilising the cell membrane of the cells at the site of electric pulse application, allowing for increased transmembrane transport of non-permeant or poorly permeant anticancer drugs, such as bleomycin or cisplatin, which possess high intrinsic cytotoxicity 1-7
Active mechanisms of electrochemotherapy
The principal mechanism of electrochemotherapy is the electroporation of cells in tumours, which increases drug effectiveness by enabling the drug to reach the intracellular targets. This increased drug uptake in tumours has been demonstrated for bleomycin and cisplatin: the accumulation of these two drugs in tumours was increased two to fourfold, compared to tumours without electroporation. 8,9 The cytotoxic effect of electrochemotherapy is not limited only to tumour cells in the tumours. Electrochemotherapy acts also on stromal cells, including endothelial cells in the lining of tumour blood vessels, resulting in their death, abrogation of tumour blood flow and consequently a cascade of tumour cell death surrounding the vessels. This vascular disrupting mechanism of electrochemotherapy contributes to its antitumour effectiveness and has been demonstrated for both bleomycin and cisplatin. 11,13 Differences in the antitumour effectiveness of electrochemotherapy were observed between immunocompetent and immunodeficient experimental animals, indicating the involvement of immune response in antitumour effectiveness. The observed tumour growth delay in immunocompetent mice was twice as long as in immunodeficient mice, and a high percentage (80%) of tumours were cured, whereas none were cured in immunodeficient mice.14 Due to massive tumour antigen shedding in organisms after electrochemotherapy, systemic immunity is induced and can be upregulated by additional treatment with biological response modifiers such as IL-2, IL-12, GM-CSF and TNF-a.4,15,16
Clinical Trials
The first clinical study was published in 1991 on head and neck tumour nodules,5 which was thereafter followed by several others.17-21 Most frequently single or multiple cutaneous or subcutaneous melanoma nodules were treated but nevertheless response was demonstrated in breast and head and neck cancer nodules, as well as Kaposi’s sarcoma, hypernephroma, chondrosarcoma and basal cell carcinoma.6 For the purpose of the present article the results of those trials have been condensed in Table 1 as studies before ESOPE trial.
Table 1 |
|||||||
Clinical response to electrochemotherapy in the ESOPE clinical trial and previous clinical studies° |
|||||||
Electrochemotherapy |
Patients |
Nodules |
Response (%) |
||||
|
PD |
NC |
PR |
CR |
OR |
||
Before ESOPE study |
247 |
1009 |
6 |
11 |
19 |
64 |
83 |
ESOPE study |
41 |
171 |
5 |
10 |
11 |
74 |
85 |
In all clinical studies reported to date, including the ESOPE study, 288 patients have been treated: 782 tumour nodules were treated by electrochemotherapy with bleomycin and 398 tumour nodules were treated by electrochemotherapy with cisplatin.
ESOPE trial
Previous clinical studies with electrochemotherapy were performed with slightly variable treatment protocols, different electrodes and different electric pulse generators. Thus there was a need for a prospective non-randomised multi-institutional study. This study was conducted by a consortium of four cancer centres gathered in the ESOPE project funded under the European Commission’s 5th Framework Programme. Treatment response after electrochemotherapy according to tumour type, drug used, route of its administration and type of electrodes was tested.22 The results of this study can be summarised as follows:
- An objective response 23 rate of 85% (73.7% complete response rate) was achieved for electrochemotherapy treated tumour nodules, regardless of tumour histology and drug or route of administration used. The cutaneous and subcutaneous nodules of melanoma were treated predominantly, breast cancer, colon cancer, squamous cell carcinoma of the skin, squamous cell carcinoma of cervix, Kaposi and leiomyosarcoma cutaneous and subcutaneous tumour nodules were treated too in decreasing sequence.
- At 150 days after treatment, the local tumour control rate for electrochemotherapy was 88% with bleomycin given intravenously, 73% with bleomycin given intratumourally and 75% with cisplatin given intratumourally, demonstrating that all three approaches were equally effective in local tumour control.
- Treatment of tumour nodules located in previously irradiated areas was equally as effective as those that were not in previously irradiated areas (objective response rate 88.2% vs. 81.4%, respectively).
- .Side effects of electrochemotherapy were minor and tolerable (muscle contractions and pain sensation). The acceptability of the treatment was demonstrated by interviewing the patients; 93% of them responded that they would be willing to accept the treatment next time if it would be indicated. The results of the ESOPE study are comparable to previously reported results on the effectiveness of electrochemotherapy (Table 1).6,22
Treatment procedure
The prerequisite for effective electrochemotherapy is a sufficient drug concentration and distribution within the tumour, as well as an adequate electric field distribution (Fig. 1).
Therefore exact procedures for either systemic or local drug delivery, using either bleomycin or cisplatin, followed by the application of electric pulses, need to be followed for each specific clinical condition. Hence, standard operating procedures (SOP) using an electric pulse generator, Cliniporator (IGEA, s.r.l. Carpi, Modena, Italy), have recently been published.25,26
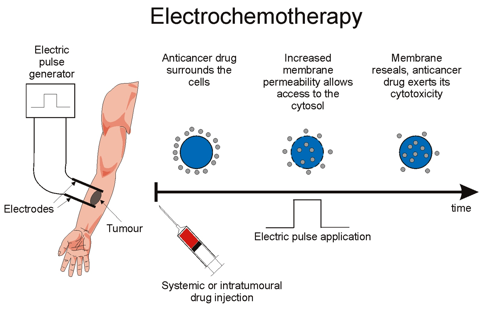
Figure 1. Principle of electrochemotherapy. Non-permeant or poorly permeant anticancer drug with intracellular target, injected either systemically or intratumourally, surrounds tumour cells. Application of adequate electric pulses causes an increase in membrane permeability, which allows for the entrance of anticancer drug into the cells to exert its cytotoxic action (redrawn from 24).
Characteristics of electric pulses
The electric pulses delivered were in most reported cases eight pulses of 100 ms duration delivered at 1 Hz, or more recently 5 kHz repetition frequency.6,30
Types of electrodes
Although there are different types of electrodes available on the market, 27 in principle two different types of electrodes exist: plate electrodes and needle electrodes. Plate electrodes are used for the treatment of skin or superficial lesions. Needle electrodes are of two kinds: needles are positioned either in two parallel rows or in a circular (hexagonal) array. In contrast to plate electrodes, needle electrodes must be inserted throughout the tumour tissue up to the deep tumour border.1,27-29
Clinical uses
Electrochemotherapy has proved to be effective in various cutaneous tumours.6,22 Currently, its main use is as a palliative treatment of cutaneous and subcutaneous tumour nodules with different histologies after all other treatment modalities have failed or proved insufficient. Most frequently it is used in the treatment of multiple cutaneous metastases of melanoma when they cannot be surgically excised due to their number or localization. In such cases long-term remission -up to several years- can be obtained (Fig. 2).19,21,30Electrochemotherapy can also be used as a cytoreductive treatment before surgical resection in an organ-sparing treatment attempted. It has been used in such a setting before a sphincter-sparing resection of anal melanoma 31 and in digital chondrosarcoma, rescuing the finger fromamputation.32Furthermore, it could be used to treat basal cell carcinoma on the face with the intent to obtain a cure. Its beneficial antitumour effects have been proved, giving better cosmetic results than excisional surgery.33
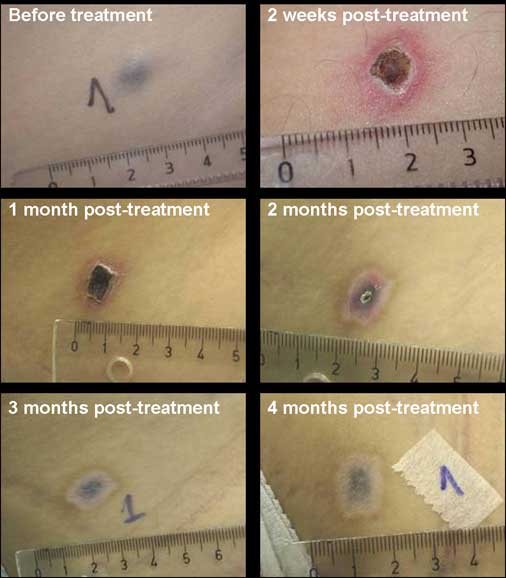
Figure 2. Typical response of melanoma nodule after treatment with electrochemotherapy. A scab forms after treatment, which exfoliates after approximately 2 months. In the treated area the pigmentation remains for a long time.
Conclusions
Electroporation-based treatments are one success story of the translation of new technology into clinical practice. Electrochemotherapy with either bleomycin or cisplatin is effective in local tumour control of cutaneous and subcutaneous tumour nodules of different histologies, resulting in up to ~75% long-term complete responses of treated tumours. After the progress of electrochemotherapy into broader clinical practice, next will be gene electrotransfer for gene therapy.
References
1. Miklavcic D, Corovic S, Pucihar G, Pavselj N. Importance of tumour coverage by sufficiently high local electric field for effective electrochemotherapy. Eur J Cancer Suppl 2006;4:45–51.
2. Miklavcic D, Semrov D, Mekid H, Mir LM. A validated model of in vivo electric field distribution in tissues for electrochemotherapy and for DNA electrotransfer for gene therapy. Biochim Biophys Acta 2000;1523:73–83.
3. Pucihar G, Kotnik T, Valic B, Miklavcic D. Numerical determination of transmembrane voltage induced on irregularly shaped cells. Ann Biomed Eng 2006;34:642–52.
4. Mir LM. Bases and rationale of the electrochemotherapy. Eur J Cancer Suppl 2006;4:38–44.
5. Mir LM, Belehradek M, Domenge C, et al. Electrochemotherapy, a new antitumor treatment: first clinical trial.CR Acad Sci III 1991;313:613–8.
6. Sersa G. The state-of-the-art of electrochemotherapy before the ESOPE study: advantages and clinical uses. Eur J Cancer Suppl 2006;4:52–9.
7. Byrne CM, Thompson JF. Role of electrochemotherapy in the treatment of metastatic melanoma and other metastatic and primary skin tumors. Expert Rev. Anticancer Ther 2006;6:671–8.
8. Belehradek Jr J, Orlowski S, Ramirez LH, Pron G, Poddevin B, Mir LM. Electropermeabilization of cells and tissues assessed by the quantitative and qualitative electroloading of bleomycin. Biochim Biophys Acta 1994;1190:155–63.
9. Cemazar M, Milacic R, Miklavcic D, Dolzan V, Sersa G. Intratumoral cisplatin administration in electrochemotherapy: antitumor effectiveness, sequence dependence and platinum content. Anticancer Drugs 1998;9:525–30.
10. Sersa G, Cemazar M, Parkins CS, Chaplin DJ. Tumour blood flow changes induced by application of electric pulses. Eur J Cancer 1999;35:672–7.
11. Sersa G, Cemazar M, Miklavcic D, Chaplin DJ. Tumor blood flow modifying effect of electrochemotherapy with bleomycin. Anticancer Res 1999;19(5B):4017–22.
12. Gehl J, Skovsgaard T, Mir LM. Vascular reactions to in vivo electroporation: characterization and consequences for drug and gene delivery. Biochim Biophys Acta 2002;1569:51–8.
13. Sersa G, Krzic M, Sentjurc M, et al. Reduced blood flow and oxygenation in SA-1 tumours after electrochemotherapy with cisplatin. Br J Cancer 2002;87:1047–54.
14. Sersa G, Miklavcic D, Cemazar M, Belehradek Jr J, Jarm T, Mir LM. Electrochemotherapy with CDDP on LPB sarcoma: comparison of the anti-tumor effectiveness in immunocompetent and immunodeficient mice. Bioelectroch Bioener 1997;43:279–83.
15. Sersa G, Cemazar M, Menart V, Gaberc-Porekar V, Miklavcic D Antitumor effectiveness of electrochemtherapy is inceased by TNF-a on SA-1 tumors in mice. Cancer Lett 1997;116:85–92.
16. Heller L, Pottinger C, Jaroszeski MJ, Gilbert R, Heller R. In vivo electroporation of plasmids encoding GM-CSF or interleukin-2 into existing B16 melanomas combined with electrochemotherapy induces long-term antitumour immunity. Melanoma Res 2000;10: 577–83.
17. Mir LM, Glass LF, Sersa G, et al. Effective treatment of cutaneous and subcutaneous malignant tumours by electrochemotherapy. Br J Cancer 1998;77:2246–42.
18. Heller R, Jaroszeski M, Perrott R, Messina J, Gilbert R. Effective treatment of B16 melanoma by direct delivery of bleomycin using electrochemotherapy. Melanoma Res 1997;7:10–8.
19. Sersa G, Stabuc B, Cemazar M, Miklavcic D, Rudolf Z. Electrochemotherapy with cisplatin: clinical experience in malignant melanoma patients. Clin Cancer Res 2000;6:863–7.
20. Bloom DC, Goldfarb PM. The role of intratumour therapy with electroporation and bleomycin in the management of advanced squamous cell carcinoma of the head and neck. Eur J Surg Oncol 2005;31: 1029–35.
21. Byrne CM, Thompson JF, Johnston H, et al. Treatment of metastatic melanoma using electroporation therapy with bleomycin (electrochemotherapy). Melanoma Res 2005;15:45–51.
22. Marty M, Sersa G, Garbay JR, et al. Electrochemotherapy e an easy, highly effective and safe treatment of cutaneous and subcutaneous metastases: results of ESOPE (European Standard Operating Procedures of Electrochemotherapy) study. Eur J Cancer Suppl 2006;4: 3–13.
23. WHO. WHO handbook for reporting results of cancer treatment. Vol 48. Geneva: WHO Offset Publications; 1997, p. 22e27.
24. Dev SB. Killing cancer cells with a combination of pulsed electric fields and chemotherapeutic agents. Cancer Watch 1994;3:12–4.
25. Mir LM, Gehl J, Sersa G, et al. Standard operating procedures of the electrochemotherapy: instructions for the use of bleomycin or cisplatin administered either systemically or locally and electric pulses delivered by the Cliniporator_ by means of invasive or non-invasive electrodes. Eur J Cancer Suppl 2006;4:14–25.
26. Domenge C, Orlowski S, Luboinski B, De Baere T, Belehradek Jr J, Mir LM. Antitumor electrochemotherapy: new advances in the clinical protocol. Cancer 1996;77:956–63.
27. Puc M, Corovic S, Flisar K, Petkovsek M, Nastran J, Miklavcic D. Techniques of signal generation required for electropermeabilization: survey of electropermeabilization devices. Bioelectrochemistry 2004; 64:113–24.
28. Pavselj N, Bregar Z, Cukjati D, Batiuskaite D, Mir LM, Miklavcic D. The course of tissue permeabilization studied on a mathematical model of a subcutaneous tumor in small animals. IEEE Trans Biomed Eng 2005;52:1373–81.
29. Snoj M, Cemazar M, Slekovec Kolar B, Sersa G. Effective treatment of multiple unresectable skin melanoma metastases by electrochemotherapy: case report. Croat Med J 2007;48:345–9.
30. Snoj M, Rudolf Z, Paulin-Kosir S, Cemazar M, Snoj R, Sersa G. Long lasting complete response in melanoma treated by electrochemotherapy. Eur J Cancer Suppl 2006;4(11):26–8.
31. Snoj M, Rudolf Z, Cemazar M, Jancar B, Sersa G. Successful sphincter-saving treatment of anorectal malignant melanoma with electrochemotherapy, local excision and adjuvant brachytherapy. AntiCancer Drugs 2005;16:345–8.
32. Shimizu T, Nikaido T, Gomyo H, et al. Electrochemotherapy of digital chondrosarcoma.J Orthop Sci 2003;8:248–51.
33. Glass LF, Fenske NA, Jaroszeski M, et al. Bleomycin-mediated electrochemotherapy of basal cell carcinoma. J Am Acad Dermatol 1996; 34:82–6.