REVIEW
A cura della Redazione della rivista “Medicina Multidisciplinare”
Successful Treatment of Penile Kaposi’s Sarcoma with Electrochemotherapy
P. CURATOLO*, M. MANCINI*, A. RUGGIERO*, R. CLERICO*, P. DI MARCO§, S. CALVIERI*
*Department of Dermatology and §Department of Anesthesia and Intensive Care Unit, University of Rome
‘‘La Sapienza,’’ Rome, Italy
Dermatol Surg 2008;34:1–5
Electrochemotherapy is a procedure that consists of the injection of low doses of highly cytotoxic drugs (like
bleomycin or cisplatin) followed up by applications of current electric pulses directly into the tumor
lesions on the skin or subcutaneous tissue, so as to improve membrane permeability and increase drug cytotoxicity.
At the appropriate pulse parameters, pore formation on the cell membrane allows low permanent drugs like bleomycin or cisplatin to enter the cell and thus locally increase thereby their toxicity: up to 10,000 times for bleomycin and 80 times for cisplatin.
In this study electrochemotherapy was performed on a patient with recurrent lesions of Kaposi’s Sarcoma (KS) on penis as an alternative treatment to surgical excision.
Fourteen months after the treatment, the patient showed no signs of local recurrency.
Case History
An 80-year-old Caucasian male was referred to our Department in January 2002 with isolated penile KS.
At first each lesion that appeared on the glans penis was treated with surgical excision.
Because of the recurrency of the local disease, he was treated with 21 cycles of chemotherapy of vinblastine sulfate intravenously (10 mg per cycle), from January 2002 to January 2006.
In June 2006, a reddish brown painful nodule, measuring 2cm in diameter on the glans penis, and numerous purplish papules, diameters ranging from 0.5 to 0.8 cm, were located on the coronal sulcus (Figure 1) of which the patient referred first manifestations 3 months before.
He refused another surgical excision, and thus he was offered the electrochemotherapy treatment.
The patient was treated under local anesthesia.
Arterial pressure, cardiac rhythm, and oximetry were continuously monitored. Bleomycin was injected intravenously at a dose of 15,000 IU/m2.
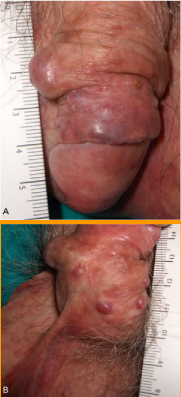
Figure 1. (A) A reddish brown nodule, measuring 2 cm in
diameter on the glans penis. (B) Numerous purplish papules,
diameters ranging from 0.5 to 0.8 cm.
The electrochemotherapy session was performed 8 minutes after the intravenous injection of bleomycin. A platinized metallic parallel electrode, 6-mm spacing, was put into contact with the skin on
both sides of the tumor lesion.
Runs of eight pulses of 680V per nodule were delivered at a frequency of 5kHz and duration of 100 μs. The electrode was placed so as to cover the entire tumor surface. The electrode and electric pulse generator (Cliniporator) were provided by IGEA S.r.l. (Carpi, Italy). After the session of treatment, the patient was kept in a recovery room for 24 hours.
Before applying electrochemotherapy and during the follow-up, each lesion was photographed and measured using a caliper.
Initially, a painless erythema and a slight edema were observed on the site of the treatment and it remained for 1 week. An ulceration began to appear within 48 to 72 hours, followed by a thick, adherent, scaly crust shortly afterward. After 4 weeks, a considerable response was observed with
complete necrosis of all the lesions treated (Figure 2).

Figure 2. After 4 weeks, complete necrosis of all the lesions treated.
At 2 months there was an excellent result with plane scars in place of treated nodules (Figure 3). Fourteen months after the treatment, the patient showed no signs of local recurrency.

Figure 3. After 2 months athrophic scar in place of treated nodules.
Discussion
Primary presentation of classic KS on the penis is uncommon and it is frequently observed in AIDS patients, who usually develop an aggressive form.
In the past 20 years, only 13 cases of primary penile non HIV-related KS have been reported in the
literature.
Treatment of primary penile KS includes local surgical excision, laser therapy, radiotherapy, and chemotherapy. Treatment with adjuvant interferon α or β has also been used.
The study suggests that electrochemotherapy of isolated penile KS is well tolerated and effective. Thus, electrochemotherapy may represent an alternative to surgical resection of recurrent cutaneous malignancies.
The advantages of this therapy are its simplicity, the short duration of treatment sessions, low doses of
chemotherapy, insignificant side effects, local tissue preservation, and improved quality of life.
Commentary
In 1872, Moriz Kaposi (1837–1902) first described the neoplasm now known as Kaposi sarcoma (KS).
A decade later Tommaso De Amicis of the University of Naples, Italy, observed a dozen more patients
with KS. Innovative work on KS continues to be performed in Italy, most recently under the inspired
leadership of Professor Stefano Calvieri and his group at the University ‘‘La Sapienza’’ in Rome employing a novel method of local chemotherapy.
In Europe and America KS in the immunocompetent is usually an indolent neoplasm. The aggressive corse first noted by Kaposi is seen with the devastation of AIDS, especially among homosexual men. KS was the original defining element of this disorder that became known as AIDS, first identified in 1981 in three reports if KS, two from New York City and one from San Francisco, before AIDS spread worldwide.
KS can occur at a wide variety of anatomic sites. Although primary penile KS is uncommon, particularly in HIV-seronegative men, this possibility has been emphasized by Micali and associates and others. Local use of cytostatic agents for KS and other cutaneous neoplasms, originally pioneered by Klein and associates in the 1960s, has been markedly expanded. Electrochemotherapy has recently been used with good results in the treatment of primary and metastatic tumors of the skin, including malignant melanoma.
This new concept of cytotoxic medication delivery appears to represent a direct and important advancement from Klein’s techniques, including his use of intralesional chemotherapy with vinblastine for KS. Facilitating entry of a cytotoxic agent such as bleomycin into the tumor cells locally with electric current to increase toxicity up to 10,000 times, especially when it can be accomplished with low-dose chemotherapy, a short duration of treatment, and insignificant side effects, is extraordinary and innovative.
The results obtained in this single case report, in which this promising treatment modality led to a prompt regression of the penile KS lesions with no relapses at a 14-month follow-up, could represent an interesting option for localized form of the disease. However, further clinical investigations in a greater number of patients are warranted.
ROBERT A. SCHWARTZ, MD, MPH
Newark, NJ
GIUSEPPE MICALI, MD
Catania, Italy